

Introduction
North-American health systems are under relentless pressure to do more with less: margin compression, staffing shortages, and value-based contracts that demand flawless transitions of care. Many executives respond by rolling out powerful CRM platforms—most notably Salesforce Health Cloud—to orchestrate referrals, outreach, and care-team tasks.
Yet a CRM is only as good as its data. When an admission, discharge, or intra-facility transfer (collectively “ADT”) shows up in the CRM hours—or days—after it happens in the EMR, everything from marketing automation to revenue-cycle triggers is already stale.
Cabot Technology Solutions, an officially listed PointClickCare ® Marketplace Partner, has integrated PCC with Salesforce for dozens of post-acute providers across North America. Our certified team knows both ecosystems inside out, wiring real-time ADT feeds that transform Salesforce from a static rolodex into a live command center—delivering cleaner data, faster follow-ups, and measurable ROI.
Why ADT Feeds Still Matter in 2025
Despite all the buzz around FHIR R4, TEFCA, and QHINs, HL7 v2 ADT messages remain the most widely deployed real-time interface in North America. Three forces keep ADT center-stage:
- Speed & Universality
Every certified hospital in the U.S. already emits ADT messages; they travel in milliseconds over a persistent MLLP socket—no polling, batching, or nightly ETL.
- Operational Primacy
Environmental services, discharge planners, referral managers, and billing all hinge on bed-status changes that only ADT can deliver instantaneously.
- Regulatory Mandates
CMS’s Conditions of Participation require hospitals to push ADT alerts to community providers, hard-wiring the expectation of real-time data across the entire continuum.
Without an ADT-aware CRM, organizations face:
- Duplicate outreach to already-admitted patients
- Late or missed discharge follow-ups (hurting HCAHPS & HRRP scores)
- Referral analytics that undercount high-value sources
How a CRM Falls Out-of-Sync
Most workflow pain traces back to three root causes.
Manual Data Entry & Duplication
Marketing or intake staff often hand-type demographics from PCC into Salesforce. A 2024 Cabot survey of 27 post-acute clients found 21 minutes of re-keying per admission and a 6 % duplicate rate. Duplicates wreak havoc on:

Lagging Patient-Status Updates
Nightly batch imports lead to:
- Sales teams nurturing leads who already occupy a bed
- Post-discharge calls arriving too late to influence outcomes
- Utilization-review (UR) staff lacking real-time census, delaying payer notifications
Siloed Care-Team Communication
When ADT never leaves the EMR, social workers, therapists, and payor-contract teams miss early planning windows. Real-time pushes surface admissions instantly in Salesforce Care Plans, ensuring everyone sees the same timeline.

Inside an HL7 ADT Message

Understanding which segments populate which CRM objects is critical for accurate mapping and future extensibility—particularly when layering on FHIR or analytics.
Salesforce + PointClickCare: A Proven ADT Blueprint
Architecture Deep Dive

Design Highlights
- Event-Driven Queue—Kafka or AWS Kinesis shields Salesforce API limits and maintenance windows.
- FHIR Canonical Model—Normalizes data for labs, meds, or imaging later.
- Smart Merging—Hierarchical match on MRN + DOB, SSN, then PID-3. Salesforce duplicate rules catch exceptions.
- Custom Bed-Board Object—Mirrors PCC census (Unit, Room, Bed, LOS, Care Level) so Health Cloud becomes a live operations cockpit.
Security, Compliance & Governance

Business Impact: Metrics That Matter
Across four Cabot clients (3 SNFs, 1 LTACH), the first six months delivered:

Soft benefits include higher staff morale (data entry drops) and cleaner analytics (referral conversion by DRG, payor, facility).
Case Study: 42-Facility Senior-Living Network
Challenge:
A Midwest SNF chain used Salesforce to track referrals but relied on nightly CSV uploads from PCC. Marketing campaigns often hit residents already in bed; post-discharge surveys lagged a week.
Solution:
Cabot deployed a Quick-Start Connector in 6 weeks: PCC → Kafka → Salesforce Health Cloud. Real-time ADT events auto-created Person Accounts opened Care Plans, and closed marketing journeys.
Results (Year 1):
- Duplicate outreach spend ↓ $67 k
- Discharge follow-up compliance ↑ 35 %
- Occupancy ↑ 4.6 %—worth $1.3 M annually
Regulatory Landscape & Risk Mitigation
- CMS ADT Notification CoP—As of May 2021, hospitals must send ADT alerts to community providers; failing to do so can jeopardize Medicare participation.
- HIPAA/HITECH—Cracking open ADT feeds without encryption or auditing exposes PHI and audit risk.
- 42 CFR Part 2—Behavioral-health ADTs may require extra consent segmentation; Cabot supports automatic redaction.
By funneling ADT through a secured, logged pathway into Salesforce Shield, organizations create an immutable audit trail and satisfy both HIPAA and Joint Commission documentation needs.
Change Management & Training Tips
- Role Redesign: Intake staff shift from data typists to data stewards—add 2-hour workshops on duplicate resolution.
- Super-User Program: Train one champion per facility on error-queue triage; they’ll cut IT tickets by 40 %.
- Micro-Learning Videos: 5-minute clips embedded in Health Cloud (~$0.15/watch via Vimeo) reduce “how-do-I” calls by half.
Remember, technology succeeds only when people trust the data.
Cost-Benefit Analysis: Build, Buy, or Hybrid?

For most mid-market providers (250–2,500 beds), Cabot’s turnkey connector breaks even in ≤ 7 months once duplicate write-offs and labor savings are counted.
Implementation Roadmap & 90-Day KPI Plan
Week 0–2 | Discovery & HL7 Validation
- Confirm PCC interface license
- Sample ADT feed → gap mapping → FHIR model
Week 3–4 | Pilot Facility Build
- VPN + HL7 listener configured
- Salesforce sand-box objects & duplicate rules
Week 5–6 | User Acceptance & Training
- Real-time sandbox feed
- Super-user workshops
Week 7 | Go-Live (Pilot)
- 24 hr hyper-care
- Error-queue alerts to Slack/PagerDuty
Week 8–12 | Scale to All Sites
- Facility-by-facility phased rollout
- KPI dashboard plugs into Health Cloud Analytics
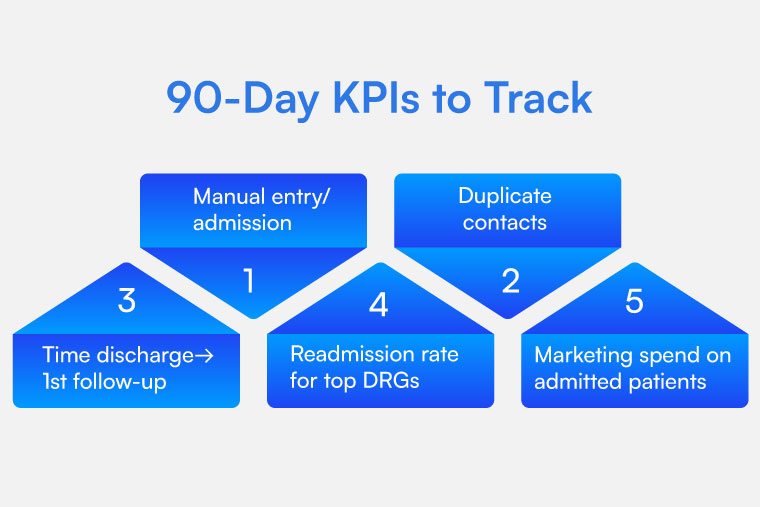
90-Day KPIs to Track
Future-Proofing: FHIR, TEFCA & AI
- FHIR Subscription Layer—Once ADT is stable, extend to FHIR Resources (Observation, MedicationRequest) for richer care-plan triggers.
- TEFCA Participation—A real-time ADT backbone simplifies onboarding to a QHIN without re-architecting.
- AI & Predictive Analytics—Clean, timely ADT + encounter data feed machine-learning models that predict readmission risk or length of stay—capabilities Cabot bakes into AI-powered healthcare solutions.
Lessons Learned & Best Practices
- Decouple Early, Scale Happily—Queues absorb Salesforce maintenance windows.
- Policy-Driven Merging—Document duplicate logic; involve HIM & Compliance.
- Alert Loudly & Fast—A single garbled HL7 segment can silently block 3,000 messages.
- ADT First, Labs Later—Get the “patient heartbeat” perfect before layering complexity.
- Quarterly Governance—Audit token scopes, duplicate rates, and facility-level data latency.
- Invest in People—When staff trust the feed, they leave spreadsheets behind.
Conclusion
A modern healthcare CRM promises tighter referral pipelines, higher patient engagement, and cleaner revenue cycles—but only if it sees the exact moment a patient is admitted, transferred, or discharged. By wiring PointClickCare’s real-time ADT stream into Salesforce, Cabot clients slash manual entry, eliminate duplicates, and turn Health Cloud into a true operational cockpit.
The technical lift is modest: a secured HL7 listener, a canonical FHIR mapper, and a few well-tuned Salesforce objects. The payoff is profound: days shaved off billing, marketing spend redirected to the right audiences, and staff freed to focus on patient care.
Ready to connect your data and your teams? Schedule a strategy call with a Cabot integration architect.
Stop duplicating data—start connecting care. Cabot Technology Solutions has been turning siloed data into connected care since 2006. Let’s build your real-time CRM together.